Congress is starving the physician-assistant workforce it just ordered to save rural healthcare.
The corporal works of mercy demand that we visit the sick, but the arithmetic of the One Big Beautiful Bill Act is designed to stop that visit before it begins. The median cost of a physician-assistant program is $103,000 for up to twenty-seven months of training, according to Sara Fletcher, executive director of the PA Education Association. The State University of New York Downstate charges $58,000 for in-state students and $113,000 for out-of-state. Physician-assistant students typically rely on federal loans to cover living expenses because the training requires sixty to eighty hours a week of classroom and clinical work, and there are no hours left to hold a job. Beginning July 1, the OBBBA caps the federal loans a physician-assistant student can borrow at $20,500 a year. There is no universe in which the loan cap covers the bill. There is no universe in which a low-income household absorbs the rest without borrowing from a private market that will not lend to it.
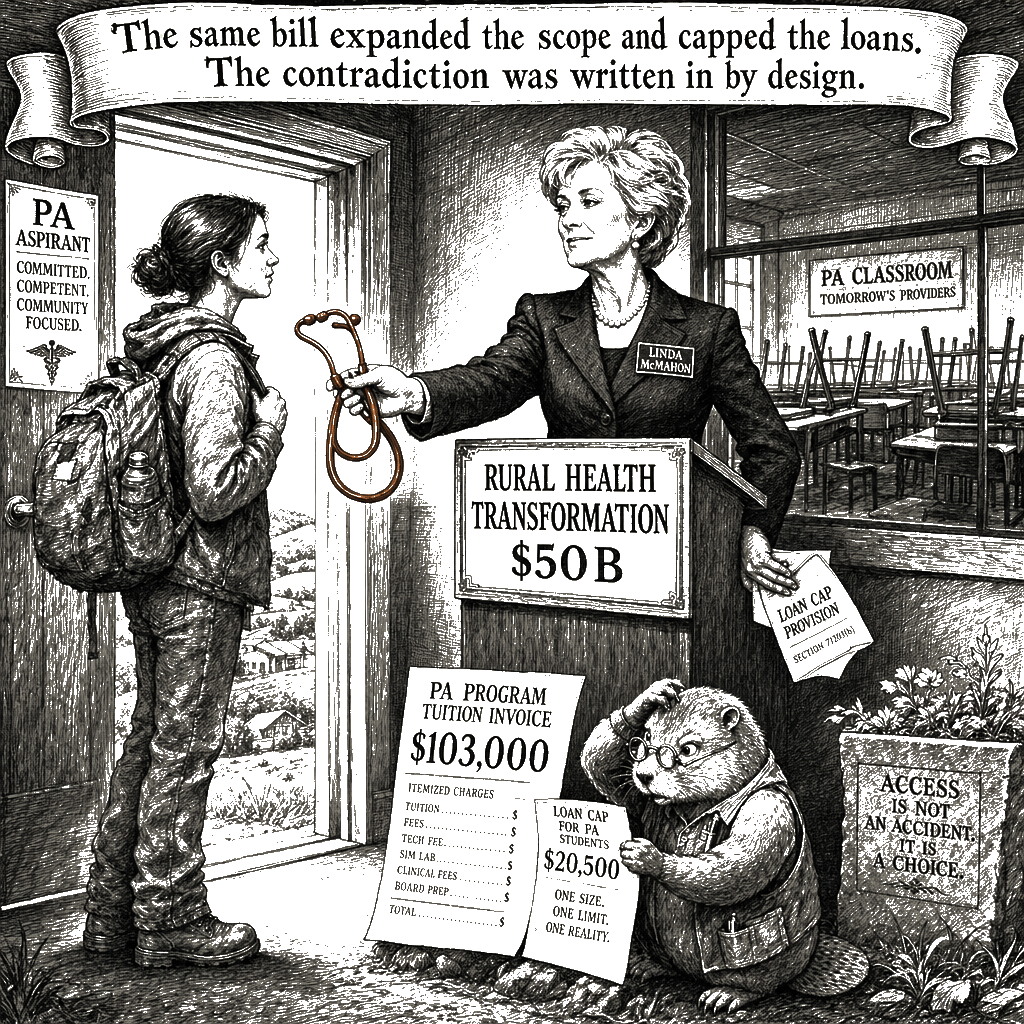
The same law that capped the loans expanded what physician assistants are permitted to do. The same law cut nearly a trillion dollars from Medicaid to pay for tax cuts, knowing the rural hospitals that depend on Medicaid revenue would be hit hardest. The same law created a $50 billion Rural Health Transformation Program, which leans, in part, on physician assistants to fill the family-medicine gaps the rural healthcare workforce cannot fill without them. The same law’s Department of Education capped the loans that pay for the training that produces the workforce the law now demands. This contradiction was not an accident. It was written into the law by design.
For students deciding whether to enroll, the math is the math. The federal graduate-and-professional loan program was built for the borrowers private lenders will not underwrite — borrowers like Todd Pickard, the president of the American Academy of Physician Associates, whose credit score was 400 when he graduated from PA school in 1997. His parents were not rich. There was nobody privately who was going to give him a dime. He graduated. He now leads the association that represents two hundred thousand physician assistants nationally. The federal program was the only door open to the students it was built for. The OBBBA closed it. The interest rates on the private loans that remain run from about three percent for borrowers with strong credit up to 17.95 percent for the rest, according to the Education Data Initiative. The borrowers the federal program was built for are precisely the borrowers the private market will not fund at any rate.
Pickard put it plainly: “I think they decided they wanted to get out of the loan business.” That is what the law wrote. The implicit message from the Department of Education is that these students are entirely on their own, and that abandonment has become the literal mission statement of the American care infrastructure. Under the new regime, a 400 credit score is a disqualifier, shunting the next generation of providers into a private debt trap.
Precarity in the United States is a policy choice, and the choice here is deliberate: shift the cost of rural healthcare from the public budget onto the private credit report. The architects of the bill know rural hospitals are collapsing, and their plan is to rely on physician assistants to fill the gap. Ten Republican-led states now employ more physician assistants than doctors. Even the White House physician is a PA — Col. James Jones, the first in the role. The math here is the same arithmetic that prompted twenty-four state attorneys general to sue to block the student loan caps for nursing and health degrees. A federal judge in Washington heard arguments a day before Pickard spoke to the press. Nursing associations, the AAPA, and the PA Education Association followed, seeking an immediate injunction. The groups expect a decision imminently.
This is what the structural looks like when it is the structural. It is not a personal failure. It is the same federal government telling physician-assistant students they will pay less for training while raising the wall around the only capital that would fund them. Education Secretary Linda McMahon told Congress the cap would bring tuition down. Sara Fletcher put it plainly: “Tuition costs are set by institutions. It’s a bigger system issue than just a PA program.” Tuition will not collapse to meet a loan cap. Loan caps will collapse to meet tuition. That is the direction of the floor.
I have the privilege of a grandmother’s estate that helped cover our Fishtown down payment, which means I am not the one staring down a 17.95 percent private loan to become a medical provider. But when I sit at my kitchen table running our household spreadsheet, I recognize the architecture. The line items refuse to balance because the system is designed to price out the people who keep rural towns alive.
The line item that does not show up in the press release about tax cuts is the body of the provider who never shows up to the clinic.# Congress Is Starving the Workforce It Demanded Save Rural America
Congress is starving the physician-assistant workforce it just ordered to save rural healthcare.
The corporal works of mercy demand that we visit the sick, but the arithmetic of the One Big Beautiful Bill Act is designed to stop that visit before it begins. The median cost of a physician-assistant program is $103,000 for up to twenty-seven months of training, according to Sara Fletcher, executive director of the PA Education Association. The State University of New York Downstate charges $58,000 for in-state students and $113,000 for out-of-state. Physician-assistant students typically rely on federal loans to cover living expenses because the training requires sixty to eighty hours a week of classroom and clinical work, and there are no hours left to hold a job. Beginning July 1, the OBBBA caps the federal loans a physician-assistant student can borrow at $20,500 a year. There is no universe in which the loan cap covers the bill. There is no universe in which a low-income household absorbs the rest without borrowing from a private market that will not lend to it.
The same law that capped the loans expanded what physician assistants are permitted to do. The same law cut nearly a trillion dollars from Medicaid to pay for tax cuts, knowing the rural hospitals that depend on Medicaid revenue would be hit hardest. The same law created a $50 billion Rural Health Transformation Program, which leans, in part, on physician assistants to fill the family-medicine gaps the rural healthcare workforce cannot fill without them. The same law’s Department of Education capped the loans that pay for the training that produces the workforce the law now demands. This contradiction was not an accident. It was written into the law by design.
For students deciding whether to enroll, the math is the math. The federal graduate-and-professional loan program was built for the borrowers private lenders will not underwrite — borrowers like Todd Pickard, the president of the American Academy of Physician Associates, whose credit score was 400 when he graduated from PA school in 1997. His parents were not rich. There was nobody privately who was going to give him a dime. He graduated. He now leads the association that represents two hundred thousand physician assistants nationally. The federal program was the only door open to the students it was built for. The OBBBA closed it. The interest rates on the private loans that remain run from about three percent for borrowers with strong credit up to 17.95 percent for the rest, according to the Education Data Initiative. The borrowers the federal program was built for are precisely the borrowers the private market will not fund at any rate.
Pickard put it plainly: “I think they decided they wanted to get out of the loan business.” That is what the law wrote. The implicit message from the Department of Education is that these students are entirely on their own, and that abandonment has become the literal mission statement of the American care infrastructure. Under the new regime, a 400 credit score is a disqualifier, shunting the next generation of providers into a private debt trap.
Precarity in the United States is a policy choice, and the choice here is deliberate: shift the cost of rural healthcare from the public budget onto the private credit report. The architects of the bill know rural hospitals are collapsing, and their plan is to rely on physician assistants to fill the gap. Ten Republican-led states now employ more physician assistants than doctors. Even the White House physician is a PA — Col. James Jones, the first in the role. The math here is the same arithmetic that prompted twenty-four state attorneys general to sue to block the student loan caps for nursing and health degrees. A federal judge in Washington heard arguments a day before Pickard spoke to the press. Nursing associations, the AAPA, and the PA Education Association followed, seeking an immediate injunction. The groups expect a decision imminently.
This is what the structural looks like when it is the structural. It is not a personal failure. It is the same federal government telling physician-assistant students they will pay less for training while raising the wall around the only capital that would fund them. Education Secretary Linda McMahon told Congress the cap would bring tuition down. Sara Fletcher put it plainly: “Tuition costs are set by institutions. It’s a bigger system issue than just a PA program.” Tuition will not collapse to meet a loan cap. Loan caps will collapse to meet tuition. That is the direction of the floor.
I have the privilege of a grandmother’s estate that helped cover our Fishtown down payment, which means I am not the one staring down a 17.95 percent private loan to become a medical provider. But when I sit at my kitchen table running our household spreadsheet, I recognize the architecture. The line items refuse to balance because the system is designed to price out the people who keep rural towns alive.
The line item that does not show up in the press release about tax cuts is the body of the provider who never shows up to the clinic.