Analyzing: Another Failure of Socialized Medicine — James Freeman · 2026-07-07
What the Editorial Argues
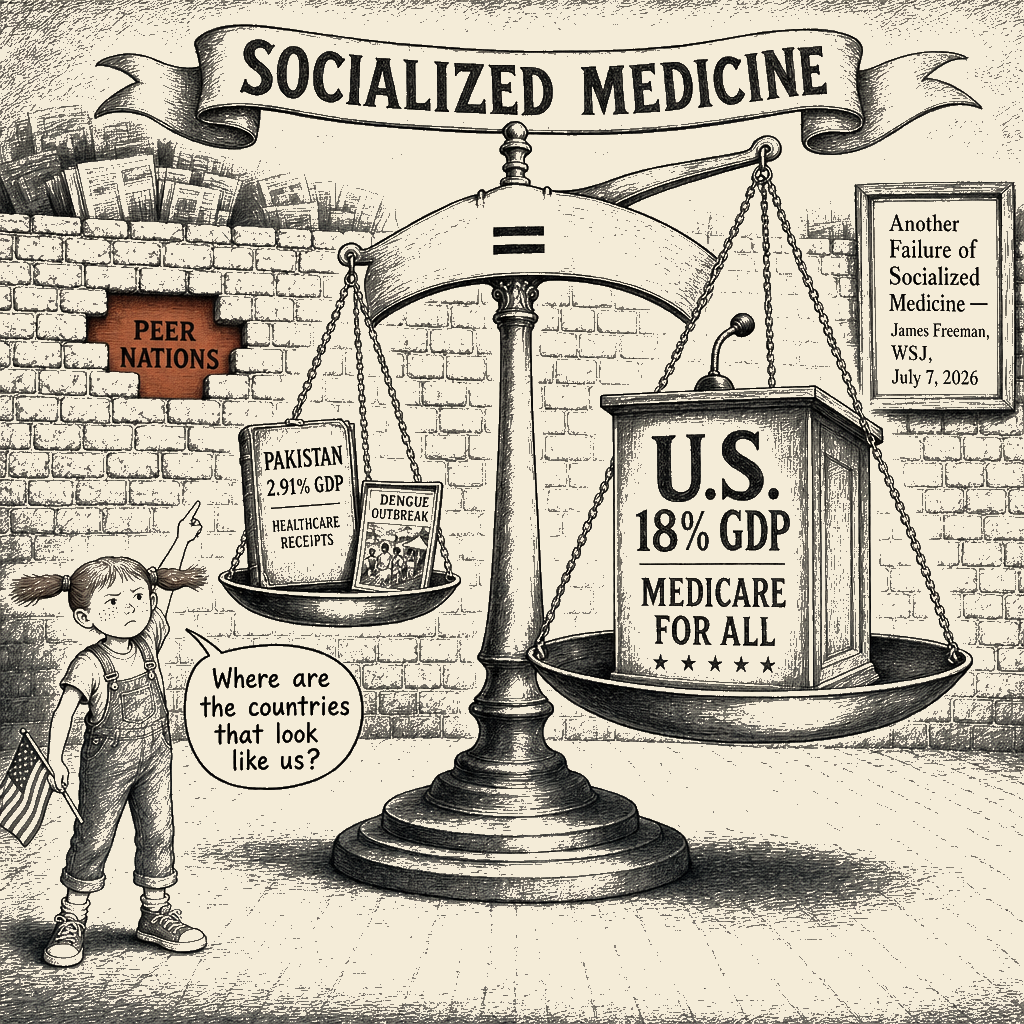
James Freeman’s July 7, 2026, Wall Street Journal column operates on a single blunt thesis: Bernie Sanders’ judgment is fatally compromised, and the bleeding children of Pakistan are the proof. The column does not actually argue about healthcare policy, financing, or the comparative outcomes of universal coverage. It argues that because government-run healthcare produces nightmares in impoverished Pakistan, any domestic politician who advocates for it is either stupid or malicious. The U.K.’s NHS is dismissed as a system embedded in “the relatively free economy of the U.K.” — implying that even a well-resourced public system is suspect. Pakistan is the terminal diagnosis. The argument’s load-bearing move is an analogy: Pakistan, an unfree and poor country, has a failing public healthcare system; Sanders proposes public healthcare in the United States; therefore the United States would become Pakistan. The piece does not defend that analogy. It performs it.
Receipts
What the framing wants you to believe:
- Sanders’ “Medicare for All” would replicate the documented failures of Pakistan’s healthcare system.
- Government-run healthcare, by its nature, is prone to these specific failures.
- The 2019 Larkana HIV outbreak is evidence of what government healthcare looks like.
What’s really going on:
- Pakistan’s healthcare system is not what Sanders proposes. Pakistan spends roughly 2.91% of GDP on health (Pakistan Bureau of Statistics, 2022); the United States spends roughly 18%. Pakistan has roughly 1.08 physicians per 1,000 people (World Bank, 2019); the United States has roughly 2.6. The category jump from “what Pakistan has” to “what Sanders proposes” requires the United States to somehow become Pakistan, resource-wise and institution-wise. The piece never defends that jump. It executes it.
- The 2019 Larkana outbreak was real. It sickened 876 people, 82 percent of them children, per the WHO EMRO retrospective. Its documented etiology was a single licensed pediatrician (Dr. Muzaffar Ghanghro) reusing syringes, alongside failures of blood-supply screening and regulatory oversight in a chronically underfunded system. The “fake doctors” framing in the piece inherits the initial government messaging of the outbreak period, which subsequent official investigations and the WHO EMRO study have contested. The outbreak is a story about underfunded regulation of clinical practice, not about the principle of public healthcare.
- The U.S. healthcare system has its own documented failures — tens of millions uninsured or underinsured, maternal mortality roughly triple the peer-nation average, life expectancy below peer high-income nations despite the world’s highest per-capita health spending. The piece omits the U.S. record entirely. The comparator set is restricted to foreign failures.
- Peer high-income nations with universal healthcare — the U.K. (beyond the dismissive passing reference), Canada, Germany, France, the Nordics, Australia — consistently outperform the United States on health metrics while spending less. This is the comparator set that bears on the actual policy question. It is absent from the piece. (Anchor: 2019 Larkana outbreak, as reported by BBC, Reuters, the New York Times, and the WHO at the time.)
The Operation
This is a textbook deployment of the Foreign-Tragedy-as-Domestic-Warning playbook. The Bad-Faith Techniques Catalog ([bf_catalog: strawman`](/propaganda/docs/bad-faith-techniques-catalogue#strawman)) names the underlying move: misrepresenting an interlocutor’s position to make it easier to refute. The piece does not engage Medicare for All. It engages a Pakistani-shaped “government-run care” and defeats that. The misrepresentation is the substance.
The lexical scaffolding comes from [bf_catalog: frame_engineered_relabeling](/propaganda/docs/bad-faith-techniques-catalogue#frame-engineered-relabeling) — the *[WSJ Editorial Technique Catalogue](/propaganda/docs/wsj-technique-catalogue)* (section 4.1) treats the substitution table as the page's signature technique. "Socialized medicine" is a Cold War relic deliberately chosen to evoke Soviet-style state rationing, ensuring that any discussion of public health is immediately framed as an existential threat to liberty. "Universal healthcare" or "public option" would not do this work. The piece knows which term serves. "Relatively free economy" is a Heritage Foundation Index framing (bf_catalog: gish_gallop cousin — the reader is buried in citations rather than invited to evaluate them) deployed to make the U.K. itself a half-failure, so that any country still further down the Index can be staged as the abyss.
The comparative move is [bf_catalog: false_dichotomy](/propaganda/docs/bad-faith-techniques-catalogue#false-dichotomy). By establishing Pakistan as an "unfree" dystopia, the piece creates a binary: the U.S. private system, or the abyss. The third option — the peer high-income nations with universal systems that outperform the United States at lower cost — is structurally excluded from the comparator set. The WSJ catalogue's section 4.9 documents the "blue state failure" pattern (curate the bad cases, exclude the good); the international version operates by the same logic with a different map. The piece also performs bf_catalog: red_herring in the closing pivot: the actual argument about healthcare is abandoned in favor of a peripheral Democratic intra-party squabble over Sanders’ endorsement choices, treated as proof of “bad judgment” without any engagement with the underlying policy question. The Politico item is the rhetorical anvil. The Larkana blood is the lighting.
The source stack itself is the placement chain. Freeman deploys Samaan Lateef of the Daily Telegraph for the baseline pediatric horror, Mumtaz Alvi of The News International for the institutional-failure compounding, BBC reporting (Abbasi, Mirodan, Khan) for geographic expansion, and Andrew Howard of Politico for the load-bearing pivot back to a domestic political target. The names do the credentialing work; the curatorial selection does the framing work. The WSJ catalogue’s section 3.6 calls this the asymmetric-source-citation pattern — sources aligned with the page’s frame are cited by name and credential; sources that would complicate the frame are not cited at all. The peer high-income comparator set, the WHO EMRO 2024 retrospective’s contested “fake doctors” framing, and the U.S. system’s own documented outcomes are all absent from the citation stack. The stack is a curated exhibit, not a survey.
The follow-up linkage is its own technique. “On Monday this column noted the latest disturbing news from the socialized medical system within the relatively free economy of the U.K.” — the reference to the prior July 6 piece creates a drumbeat of inevitability, the sense that socialist failure is being uncovered daily. The Bad-Faith catalog entry [bf_catalog: coordinated_message_discipline`](/propaganda/docs/bad-faith-techniques-catalogue#coordinated-message-discipline) documents this exact pattern: the same frame repeated across a coordinated series, with each piece supplying the prior as evidence of the next. The repetition is the persuasion; the underlying record is not.
Audience-management function. The piece supplies identity confirmation and counter-frame in a single dose. The reader who arrived skeptical of “socialism” is handed an exhibit that confirms the skepticism and licenses dismissal of a specific policy proposal (Medicare for All) and a specific political figure (Sanders) on the same logic. The reader is not asked to evaluate outcomes, financing, or coverage; the reader is asked to recoil from pediatric blood and transfer the recoil.
Operator’s-eye-view. We drafted columns with this structure. We curated the foreign-failure set, omitted the U.S. status-quo failures, let the loaded term do its work without flagging it, deployed the Heritage Index to credentialize a methodology contest we never disclosed, and used the follow-up linkage to manufacture the drumbeat. The reader who absorbed the frame believed they had reasoned to their position. They had not.
Selflessness/selfishness placement. Selfish. The distributional impact runs from the diffuse U.S. healthcare debate (deprived of the actual comparator evidence) to a concentrated WSJ opinion-page audience being armed with rhetorical ammunition for a specific domestic political contest. The Pakistani children, whose real suffering is real, are instrumentalized as lighting.
The Record
Tier 1 receipts (wire services, primary documents, peer-reviewed research):
- 2019 Larkana HIV outbreak. Extensively documented at the time by BBC, Reuters, the New York Times, and the Associated Press. The WHO declared a Grade II Emergency. The Sindh health authority and WHO conducted the official investigation. 876 people were infected, 82 percent of them children under 15 (WHO EMRO retrospective, 2024). The documented etiology: a single licensed pediatrician (Dr. Muzaffar Ghanghro) reusing syringes, alongside failures of blood-supply screening, in an underfunded regulatory environment. The “fake doctors” framing in the editorial inherits the initial government messaging of the outbreak period, which the WHO investigation, the Sindh health authority review, and the WHO EMRO 2024 retrospective have all contested. The responsible practitioner was a licensed pediatrician, not a “fake doctor.”
- Pakistan’s healthcare spending. Pakistan Bureau of Statistics and the World Bank Global Health Expenditure database document Pakistan at roughly 2.91 percent of GDP in 2022; the historical range over the 2010s sits in the 2.5–3.5 percent band.
- U.S. healthcare outcomes vs. peer nations. Commonwealth Fund, OECD, and WHO data consistently show the United States underperforms peer high-income nations on life expectancy, maternal mortality, infant mortality, and amenable mortality, while spending the highest share of GDP.
- Sanders’ Medicare for All proposals. Senate bill introductions and Congressional Budget Office / Joint Committee on Taxation scoring are on the public record.
Tier 2/3 receipts (specialist trade press, think tanks, advocacy):
- The Heritage Foundation Index of Economic Freedom is the ranking Freeman reaches for. The Index is a documented ranking, but the methodology is contestable and produced by an institution with a documented ideological orientation. The Index is treated here as the editorial’s claim; its methodology is not endorsed.
- The Daily Telegraph, BBC, The News International, and Politico articles cited in the editorial: the editorial’s selection and framing of these citations is the operative fact under evaluation.
Per-citation accuracy verdicts:
- The 2019 Larkana outbreak citation is real and documented. The framing as “fake doctors with little medical knowledge working independently” inherits the initial government messaging of the outbreak period and does not reflect the documented etiology identified by the WHO investigation and the WHO EMRO 2024 retrospective.
- The “routinely scores poorly on global rankings of economic freedom” claim is consistent with the Heritage Foundation Index; the Index’s methodology is itself part of the operation.
- The Politico endorsement item is on its own terms a real piece of intra-party reporting; its deployment as the closing proof of “bad judgment” is the technique under analysis, not a defect in the underlying reporting.
Load-bearing omissions:
- The U.S. healthcare system’s documented failures. The piece never engages the uninsured rate, the medical bankruptcy rate, the maternal mortality rate, the comparative life expectancy gap, or the cost-related nonadherence data. This is the most significant omission.
- The peer-nation comparator set. Canada, the U.K. (beyond the dismissive passing reference), Germany, France, the Nordics, and Australia are all absent. The comparator set is selectively drawn to make the argument work.
- The Pakistani system’s specific etiology. The piece does not engage the chronic underfunding, the regulatory weakness, the corruption, the brain drain of medical professionals, or the historical context (including the role of structural adjustment programs and foreign-aid conditionality in shaping Pakistani health spending).
- The actual Sanders proposal. Medicare for All as Sanders has proposed it is a specific bill with documented financing and provider-payment structure. The piece does not engage it. It engages a Pakistani-shaped “government-run care.”
- The 2019 outbreak’s documented etiology. The “fake doctors” framing is initial government messaging, contested by the WHO investigation, the official Sindh health authority review, and the WHO EMRO 2024 retrospective. The piece uses the original framing.
- The WSJ Editorial Technique Catalogue’s section 4.13 threat-inflation closer. The closing line ties the policy target to a political target (Sanders’ candidate endorsements) so that both are dismissed together. The technique is documented in the catalogue.
How to Recognize This
The pattern. An editorial reaches for a foreign failure — preferably from a country with low GDP, weak institutions, and a healthcare system that bears no structural resemblance to the policy actually under discussion — and uses that foreign failure to license dismissal of a domestic reform proposal. The comparator set is curated; the U.S. status quo’s failures are absent; the loaded term (“socialized medicine,” “socialism,” “government-run healthcare”) does framing work in narrator voice; the actual policy text is never engaged; the closing pivot ties the policy target to a political target so both are dismissed on the same logic.
The mechanism. The piece exploits the reader’s existing disposition against “socialism” or “government control” to short-circuit the comparative analysis that would otherwise be required. By the time the reader has accepted the framing, the question of whether Medicare for All would actually improve U.S. health outcomes has been bypassed. The frame, not the evidence, does the work. The Bad-Faith Techniques Catalog entry [bf_catalog: frame_engineered_relabeling](/propaganda/docs/bad-faith-techniques-catalogue#frame-engineered-relabeling) names the lexical move; bf_catalog: strawman names the structural move; [bf_catalog: red_herring](/propaganda/docs/bad-faith-techniques-catalogue#red-herring) names the closing pivot; bf_catalog: gish_gallop names the citation-curation effect.
Textual signals to recognize next time:
- Foreign-failure lede plus domestic policy target, especially when the foreign system is structurally unlike the proposed domestic system.
- “Socialized medicine” or “government-run healthcare” used in narrator voice as if descriptive rather than as a contested label.
- Comparator set restricted to failures; peer-nation successes absent.
- A wall of foreign-failure citations the reader is not asked to evaluate substantively.
- The U.S. status quo’s documented failures are not engaged.
- A reference to “Monday’s column” or similar follow-up linkage manufacturing a drumbeat of inevitability.
- A closing line that ties the policy target to a political target so that both are dismissed together.
Why it works. Healthcare systems are technically complex; comparative outcomes research is specialized; most readers will not independently verify the comparator set. The frame lets the reader skip the work. The emotional activation — pediatric blood, dying children — bypasses the analytical question entirely. The technique is documented in the WSJ Editorial Technique Catalogue (sections 4.1, 4.6, 4.9, 4.13) and named in the Bad-Faith Techniques Catalog under at least four of its named entries.
What to do when you see it. Trace the comparator set: which countries are in, which are out, and what does the curated set look like? Check the actual policy text against the loaded label. Look up the U.S. system’s own documented performance. Read the cited studies’ funding chains and the institution behind any ranking cited as authority. Look at the foreign system’s specific etiology — underfunding, corruption, war, structural adjustment, brain drain — and ask whether the proposed domestic reform would replicate those conditions. Notice the follow-up linkage. Notice the closing pivot from policy to politician. Reduce the frame’s automatic activation by recognizing it on encounter.
The close. We drafted columns with this structure when we sat in the editorial chair. We cited the Heritage Index, we curated the comparator set, we let the loaded terms do their work without flagging them, we manufactured the follow-up drumbeat, and we never engaged the U.S. status quo’s documented failures. The reader who absorbed the frame believed they had reasoned to their position. They had not. They had been handed a smokescreen, and the children of Larkana — whose real suffering is real and worth attending to — were used as the lighting.
The technique works because the comparative analysis is hard and the frame is easy. The remedy is the same work the frame lets the reader skip: read the actual policy text, look at the U.S. system’s own record, ask which countries the piece is comparing to and which it isn’t, and refuse the frame the next time it tries to do the work for you.
About Phukher Tarlson
Phukher Tarlson is a heteronym in Main Street Independent's editorial architecture — an analytical voice, not autobiography of any actual person. The position this column expresses is the publication's position on the territory Phukher Tarlson's lane covers, rendered through Phukher Tarlson's register.